

IOL power calculation formulas
IOL calculation formulas explained
When planning cataract surgery, one of the most crucial stages for treatment success is choosing the correct intraocular lens (IOL) power.1 To reach the targeted refraction, the selection must be performed according to the anatomical and optical parameters of the eye.2 In most cases, the target refraction is emmetropia but in some cases, depending on the specific needs and demands of the individual patient, other targets might be required, such as leaving some level of residual myopia in one eye (monovision).3 One of the most important parameters in IOL calculation, particularly in non-syndromic myopia, is axial length (AL). AL is a combination of anterior chamber depth (ACD), lens thickness and vitreous chamber depth and can change the IOL power by up to 2.5 to 3 times. [Meng 2011, Eyewiki] Corneal power is another important component of IOL power determination and keratometry (K) is the measurement of the corneal radius of curvature. The cornea is the transparent part of the eye that covers the iris, pupil and anterior chamber and it accounts for around two thirds of the eye's total optical power. Changes in corneal power can alter the IOL power in a ratio of nearly 1:1. As well as AL and K, other parameters that may be also required, depending on the type of formula used, are the preoperative ACD5 and the corneal white-to-white distance (WTW; also called the horizontal corneal diameter).6 The anterior chamber is the fluid-filled space between the iris and the innermost surface of the cornea and the WTW distance is the horizontal distance between the borders of the corneal limbus.
What is the effective lens position?
The only parameter that cannot be measured preoperatively is the position where the IOL "settles down" after surgery, which is also known as the effective lens position (ELP). Prediction of this parameter is initially performed by the IOL manufacturer in form of the A-constant. The A-constant is an empirical value and is specific to the design of the IOL. This constant is later refined by statistical optimizations that reflect the variance of the patient's particular preoperative biometry, and the surgeon's personal surgical technique is also taken into account. ELP is defined as the effective distance between the anterior surface of the cornea and the lens plane if the lens was infinitely thin.4,5 The ELP is considered to be the main limiting factor for refractive predictability after cataract surgery, as the accuracy of AL and corneal power measurements has been widely demonstrated.7 Improvements in IOL power calculations over the past 30 years are the result of improved predictability of the ELP variable.
Mathematical formulas have been developed for best estimation of the ELP, most of which are based on paraxial optics (Figure 1).2,4 In these formulas, some ocular parameters are required and the surgeon should know the intended target refraction.2,4
What are the differences between the IOL formulas?
Many published and unpublished IOL formulas are available. The most frequently used formulas are based on two measurements, AL and K, as well as a single IOL constant8 (Holladay 1,9 SRK/T10 and Hoffer Q11). Predictions of ACD, which increases relative to the increase of AL, are based on initial and generally large datasets from which the formulas have been derived; however individual ACD measurements were not included in the prediction model. The Haigis formula therefore uses three measurements, AL, K and pre-operative ACD with the three IOL constants a0, a1 and a2.12 Olsen's formula is based on two additional measurements - pre-operative refraction and lens thickness - and delivers one IOL constant whereas the Holladay 2 formula is based on seven measurements, including the patient's age and the horizontal WTW measurement.1,5 Finally, the Barrett formula uses a theoretical model eye whereby ACD is related to AL and K, and is also determined by the relationship between the A-constant and a ‘lens factor'. The position of the principle plane of the IOL is kept as a relevant variable.13
|
SRKI/II, SRK/T, manufacturer
|
Holladay 1
|
Hoffer Q
|
Haigis
|
|
A-constant
|
sf (surgeon factor)
|
pACD
|
a0, a1, a2
|

Which formula to use for which eye (length)?
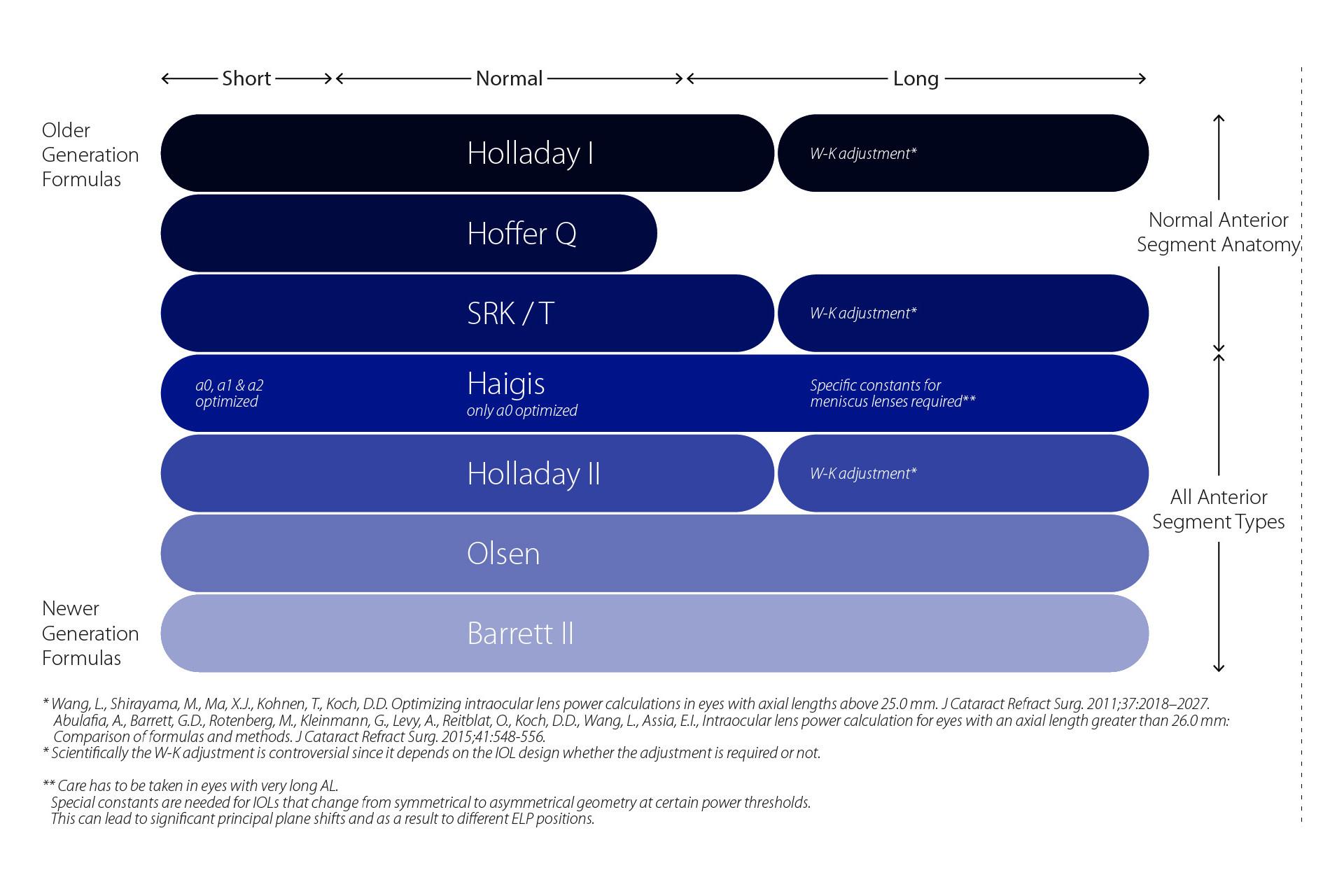
For normal ALs of 22.5 to 24.5 mm most formulas work well with minimal discrepancies. In 199311 and again in 2000,14 Hoffer performed studies to analyse which formula was the most accurate for ALs of a shorter or longer length than normal. These studies concluded that the Hoffer Q formula provided the most reliable results in short eyes (AL < 22.0 mm) while the SRK/T formula was best in long eyes (AL > 26.0 mm).11,14 Recently, in a database study of 8,108 eyes undergoing cataract surgery, the Hoffer Q formula was found to provide the best refractive outcomes in eyes shorter than 21.00 mm and the Holladay 1 and Hoffer Q formulas were equally reliable for eyes with an AL between 21.00 mm and 21.49 mm.15 This same study also concluded that the Holladay 1 formula may perform marginally better for eyes between 23.50 mm and 25.99 mm, although the Hoffer Q, Holladay I and SRK-T formulas gave comparable refractive outcomes.14 Finally, these authors found that the SRK/T formula performed significantly better for eyes with an AL of 27.00 mm or longer.15 For highly myopic eyes the Barrett II formula may be a suitable choice and other studies have demonstrated the high level of accuracy of the Haigis formula in extreme hyperopia.16 ,17 See Figure 1.
In conclusion, calculation of the IOL power can be performed using a great variety of formulas. According to clinical studies, the SRK-T formula is recommended for rather long eyes whereas the Hoffer Q formula is recommended for rather short eyes. The Holladay 1 and Hoffer Q formulas are equally good for eyes with an AL between 21.00 mm and 21.49 mm and the Holladay 1 formula seems to perform better than the Hoffer Q formula for eyes between 23.50 mm and 25.99 mm. Fourth generation formulas, like the Barrett, Haigis or Holladay 2 formula, have the advantage of including the non-proportional relationship between the ACD and AL and therefore should provide the highest accuracy over the full range of ALs.
Formulas for IOL Power Calculation
Which modern intraocular lens (IOL) calculation formula gives the best results for prediction of the effective lens position (ELP) is a widely debated topic. In this section you'll find an overview of the latest generation of formulas for rotationally symmetrical IOL designs (post-laser vision correction eyes are excluded) with their philosophy explained in a nutshell. Furthermore the parameters of each formula used for the ELP prediction are listed as well as recommendations of formulas for different eye types according to various sources.
-
The Barrett Universal 2 formula uses a theoretical model eye in which anterior chamber depth (ACD) is elated to axial length (AL) and keratometry. A relationship between the A-constant and a "lens factor" is also used to determine ACD.19 The important difference between the Barrett formula and other formulas is that the location of the principle plane of refraction of the IOL is retained as a relevant variable in the formula.
Parameters used for ELP prediction
AL, corneal power, ACD (optional), lens thickness (optional), white-to-white corneal diameter (optional).
Recommended eye type
The Barrett formula is recommended for short – long eyes.20
-
The Haigis formula recommends an IOL power based on a three-variable (a0, a1 and a2) function. The a1 constant is tied to the measured ACD, while the a2 constant is tied to the measured AL. This allows all three constants to be optimized for a wide range of ALs and ACDs using double-regression analysis.
Parameters used for ELP prediction
These are AL and ACD.
Recommended eye type
Haigis (a0 optimized only): normal eyes20
Haigis (a0, a1, a2 optimized): short – long eyes20,* -
The Hoffer Q formula relies on a personalized ACD, AL and corneal curvature. The personalized ACD (pACD) is developed from any given series of a particular IOL style. It includes (1) a factor that increases the ACD with increasing AL, (2) a factor that increases the ACD with increasing corneal curvature, (3) a factor that moderates the change in ACD for extremely long and short eyes, and (4) a constant added to the ACD.21
Parameters used for ELP prediction
These are AL and corneal power.
Recommended eye type
The Hoffer Q formula should be used for eyes measuring < 22 mm, according to the Royal College of Ophthalmology guidelines.22
-
The Holladay 1 formula uses the postoperative stabilized refraction value, the dioptric power of the implanted IOL, and the preoperative corneal and AL measurements to calculate a personalized surgeon factor. Thus, the surgeon factor is defined as the distance from the post-operative anterior iris plane to the effective optical plane of the IOL. As with other constants the surgeon factor is not actually a measurement, but a number representing a particular surgeon's previous experience.23
Parameters used for ELP prediction
These are AL and corneal power.
Recommended eye type
The Holladay 1 is recommended for eyes measuring between 24.6 mm – 26.0 mm.22
-
The Holladay 2 formula is conceptually based on the Holladay 1 formula; however it uses seven parameters for predicting the surgeon factor. These are the AL, corneal power, ACD, lens thickness, age, white-to-white corneal diameter and pre-operative refraction data. How the formula works in detail has not yet been revealed by Jack Holladay.
Parameters used for ELP prediction
These are AL, corneal power, ACD, lens thickness (optional), age (optional), white to-white corneal diameter (optional), pre-operative refraction data (optional).
Recommended eye type
The Holladay 2 formula is recommended for short – long* eyes.20
*W-K adjustment has been shown to extend the usage from "short – normal eyes" to "short – long eyes" for meniscus IOLs designs in the low plus to minus power range.24
-
The SRK/T formula is a theoretical (T) approach to IOL power calculation under the SRK umbrella of empirical formulas using existing A-constants and optimization methods. Empirical optimization methods of the SRK/T model primarily consist of (1) postoperative ACD prediction, (2), a retina thickness correction factor and (3) corneal refractive index.25
Parameters for ELP prediction
These are AL and corneal power.
Recommended eye type
The SRK/T formula should be used for eyes > 26 mm. A combination of Hoffer Q, Holladay 1, and SRK/T should be used for eyes 22.0–24.5 mm.22
-
The SRK I and SRK II formulas are obsolete and should no longer be used.26
-
1
Lee AC, Qazi MA, Pepose JS. Biometry and intraocular lens power calculation. Curr Opin Ophthalmol 2008; 19: 13-7.
-
2
Hoffer KJ. IOL power. Thorofare, NJ, USA: Slack Incorporated, 2011.
-
3
Beiko GH. Comparison of visual results with accommodating intraocular lenses versus mini-monovision with a monofocal intraocular lens. J Cataract Refract Surg 2013; 39: 48-55.
-
4
Shammas HJ. Intraocular lens power calculations. Thorofare, NJ, USA: Slack Incorporated, 2004.
-
5
Olsen T. Prediction of the effective postoperative (intraocular lens) anterior chamber depth. J Cataract Refract Surg 2006; 32: 419-24.
-
6
Fenzl RE, Gills JP, Cherchio M. Refractive and visual outcome of hyperopic cataract cases operated on before and after implementation of the Holladay II formula. Ophthalmology 1998; 105: 1759-64.
-
7
Shammas HJ, Chan S. Precision of biometry, keratometry, and refractive measurements with a partial coherence interferometry-keratometry device. J Cataract Refract Surg 2010; 36: 1474-8.
-
8
Haigis W. Matrix-optical representation of currently used intraocular lens power formulas. J Refract Surg 2009; 25: 229-34.
-
9
Holladay JT, Prager TC, Chandler TY, Musgrove KH, Lewis JW, Ruiz RS. A three-part system for refining intraocular lens power calculations. J Cataract Refract Surg 1988; 14: 17-24.
-
10
Retzlaff JA, Sanders DR, Kraff MC. Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg 1990; 16: 333-40; correction, 528.
-
11
Hoffer KJ. The Hoffer Q formula: a comparison of theoretic and regression formulas. J Cataract Refract Surg 1993; 19: 700-12; errata 1994; 20: 677.
-
12
Haigis W, Lege B, Miller N, Schneider B. Comparison of immersion ultrasound biometry and partial coherence interferometry for intraocular lens calculation according to Haigis. Graefes Arch Clin Exp Ophthalmol 2000; 239: 765–773.
-
13
Barrett GD. An improved universal theoretical formula for intraocular lens power prediction. J Cataract Refract Surg. 1993 Nov;19(6):713-20.
-
14
Hoffer KJ. Clinical results using the Holladay 2 intraocular lens power formula. J Cataract Refract Surg 2000; 26: 1233-7.
-
15
Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refract Surg 2011; 37: 63-71.
-
16
Zhang Y, Ying Liang X, Liu S, Lee JWY, Bhaskar S, Lam DSC. Accuracy of intraocular lens power calculation formulas for highly myopic eyes. J Ophthalmol 2016. doi: 10.1155/2016/1917268.
-
17
MacLaren RE, Bourne RR, Restori M, Allan BD. Biometry and formula accuracy with intraocular lenses used for cataract surgery in extreme hyperopia. Am J Ophthalmol 2007; 143: 920-31.
-
18
http://www.doctor-hill.com/iol-main/formulas.htm Accessed 26 September 2016.
-
19
An improved universal theoretical formula for intraocular lens power prediction. Barrett GD. J Cataract Refract Surg. 1993 Nov;19(6):713-20.
-
20
IOL Power Calculations Which Formula? http://www.doctor-hill.com/iol-main/formulas.htm.
-
21
The Hoffer Q formula: A comparison of theoretic and regression formulas Kenneth J. Hoffer, M.D. J CATARACT REFRACT SURG-VOL 19, NOVEMBER 1993.
-
22
The Royal College of Ophthalmologists Cataract Surgery Guidelines September 2010 Scientific Department The Royal College of Ophthalmologists. https://www.rcophth.ac.uk/wp-content/uploads/2014/12/2010-SCI-069-Cataract-Surgery-Guidelines-2010-SEPTEMBER-2010.pdf
-
23
A three-part system for refining intraocular lens power calculations Jack T. Holladay, M. D. Thomas C. Prager, Ph.D. Thomas Y. Chandler, M. D. Kathryn H. Musgrove, M.D. John W. Lewis, M.D. Richard S. Ruiz, M.D. J CATARACT REFRACT SURG-VOL 14, JANUARY 1988.
-
24
Optimizing intraocular lens power calculations in eyes with axial lengths above 25.0 mm Li Wang, MD, PhD, Mariko Shirayama, MD, Xingxuan Jack Ma, Thomas Kohnen, MD, PhD, FEBO, Douglas D. Koch, MD J Cataract Refract Surg 2011; 37:2018–2027
-
25
Development of the SRK/T intraocular lens implant power calculation formula John A. Retzlaff, M.D., Donald R. Sanders, M.D., Ph.D., Manus C. Kraff, M.D. J CATARACT REFRACT SURG-VOL 16, MAY 1990.
-
26
Nemeth J, Fekete O, Pesztenlehrer N. Optical and ultrasound measurement of axial length and anterior chamber depth for intraocular lens power calculation. J Cataract Refract Surg 2003; 29(1):85-8.