Laying the Foundation for Success in Cataract Surgery with State-of-the-Art Technology, Part 2
Anterior chamber stability and safe cataract surgery

Numerous factors contribute to success in cataract surgery and influence the experience for patients, surgeons, and their surgical team. In this four-part interactive program, leading cataract surgeons provide insights on strategies for optimizing outcomes in cataract surgery. It begins with tips for a proper preoperative evaluation that will help surgeons plan the procedure, minimize the risk of intraoperative complications, and achieve the desired visual results. The rest of the program is devoted to developments in technology that improve safety, efficacy, and efficiency.
Part 2: Anterior chamber stability and safe cataract surgery
Over the past 50 years, phacoemulsification machines have undergone a constant process of improvement, and this evolutionary process has consisted of numerous incremental upgrades. In particular, there has been attention to developing advanced fluidics systems that will maintain intraocular pressure (IOP) control and anterior chamber stability with the aims of reducing intraoperative complications, improving surgical outcomes, and increasing patient satisfaction.
What’s new in phacoemulsification
The ZEISS QUATERA 700 is the latest entry into the space of modern phacoemulsification systems with advanced fluidics. I was involved in the development of the device, which took place over a period of about 5 years, and I have used it to perform over 1000 cases. In my opinion, the QUATERA 700 stands out from the competition for a variety of reasons, but particularly because of its novel patented QUATTRO pump (Figure 3). Neither a peristaltic nor a venturi system, the QUATTRO pump is a membrane pump operating via four syringe-like chambers that provide synchronized and reciprocal exchange of infusion and aspiration. It has two infusion chambers that variably control infusion rate and two aspiration chambers that control the aspiration and vacuum levels. The pump’s sensors measure actual irrigation and aspiration fluid volume, and the technology automatically and quickly compensates for incision leakage to maintain the preset IOP and a very stable anterior chamber.
The IOP can be set between 30 mmHg and 120 mmHg. Using the QUATERA 700, I usually set IOP at 40 mmHg or 50 mmHg. Even in cases where there is excessive leaking from a wide incision, I have not experienced surge because the QUATTRO pump compensates for the leakage (Figure 4).
As a nice convenience when operating with the QUATERA 700, I am able to use BSS that comes in either a bag or a bottle. Some other phacoemulsification machines accommodate only a bag or only a bottle. For example, the Centurion Vision System (Alcon), which features a peristaltic pump with active fluidics, can only use a specific BSS bag from the device manufacturer because the container has to be compressed between two metal plates to provide forced infusion. The Stellaris (Bausch+Lomb) has a vacuum-based pump that uses forced infusion from a rigid bottle through a connected air pump. Furthermore, these systems as well as the WHITESTAR SIGNATURE PRO (Johnson & Johnson Vision), which features both peristaltic and venturi pumps and can use either a bag or bottle for gravity driven passive fluid infusion, provide only an approximate increase in irrigation to compensate for surge because they do not directly measure the volume of fluid infused versus the volume of fluid aspirated, and they do not have mechanisms to compensate for incision leaks.
Surgical efficiency, safety and convenience
In addition to its QUATTRO pump, the QUATERA 700 has other features that I find helpful for enhancing my surgical safety, efficiency, and convenience.These include innovative technology for ultrasound management that helps to reduce ultrasound energy usage. Known as Power on Demand (POD), this advanced technology automatically activates ultrasound power upon occlusion of the aspiration hole with nuclear material and automatically deactivates ultrasound once the occlusion is cleared.
Therefore, when removing fragments, surgeons using the QUATERA 700 can keep the phacoemulsification tip in the center of the anterior chamber and press the foot pedal all the way down because phacoemulsification will only be activated once the fragment comes to the tip and occludes the aspiration hole. Using POD, surgeons can concentrate on what is going on inside the eye. Eliminating the need to think about pressing and releasing the foot pedal to modulate ultrasound delivery reduces the stress of the surgical experience for me. I find POD is particularly useful for cases with harder cataracts where there is a need to limit the amount of ultrasound, but in my opinion it is also helpful for preventing beginning surgeons from using too much ultrasound when operating on soft cataracts. I think that inexperienced surgeons have a habit of using ultrasound unnecessarily in these cases, and POD addresses that situation by limiting ultrasound activation to times of fragment occlusion.
Compatibility with the ZEISS CALLISTO eye system and the ZEISS FORUM is another feature of the QUATERA 700 that I greatly appreciate in my daily routine because I believe this integration enables more controlled and efficient surgery. Please refer to the section titled “The advantages of a digital workplace in modern cataract surgery” by Dr Florian Kretz for detailed information on his streamlined digital workflow.
Comparative clinical evaluation
To confirm my clinical impressions about the surgical performance and safety of QUATERA 700, I conducted a single surgeon clinical study randomizing eyes to undergo surgery using the QUATERA 700, Centurion Vision System, or WHITESTAR SIGNATURE PRO . The primary aim of the study was to compare anterior chamber stability using the different platforms, but we also looked at surgical efficiency (effective phaco time and total phaco time, time taken per case according to nucleus grade), incidence of intraoperative complications, and corneal parameters as an indicator of ultrasound usage.
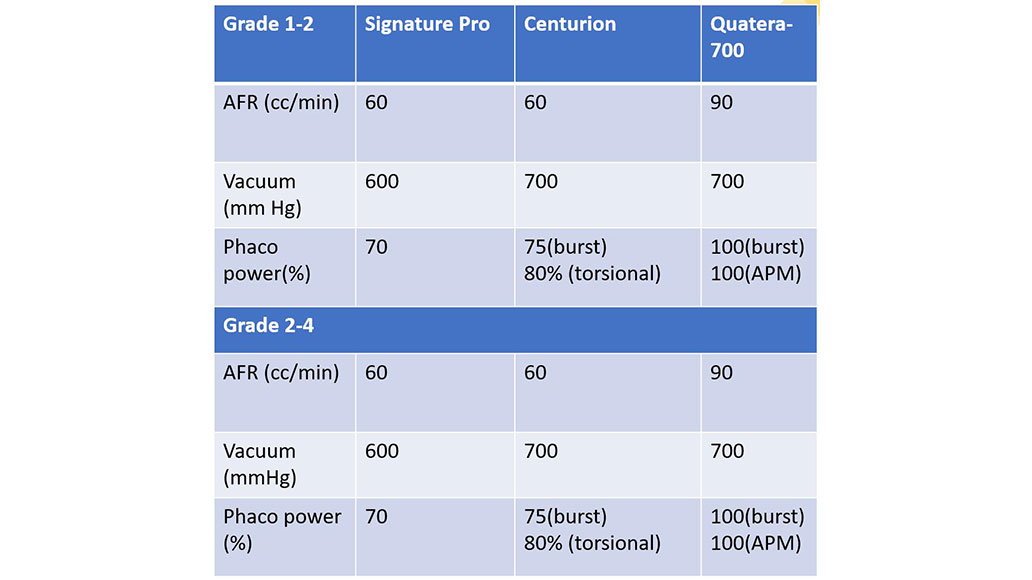
The study included 90 eyes with a soft cataract (LOCS 1 to 2) and 90 eyes with a dense cataract (LOCS 2+ to 4). In all cases, phacoemulsification was performed through a 2.2 mm clear corneal incision using a direct chop technique and with machine parameters chosen as the maximum for each platform (Table 1). All eyes received the same model foldable posterior chamber IOL.


Data for each phacoemulsification system were analyzed separately for the subgroups of eyes with soft and dense cataracts. Preoperatively, there were no statistically significant differences in age, axial length, keratometry, anterior chamber depth, central corneal thickness, endothelial cell count, or IOL power comparing the different phacoemulsification machine groups within either the soft or dense cataract subgroups.
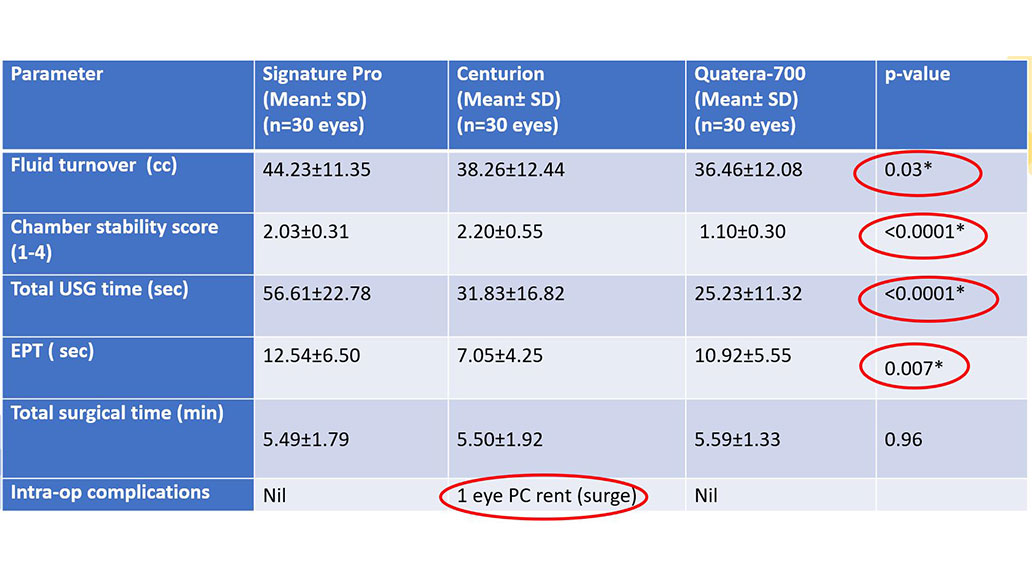
Detailed results from the study will be reported in a planned publication. Table 2 shows findings from analyses of intraoperative parameters for the dense cataract group. Using a four-point scale to grade anterior chamber stability (Grade 1 = excellent chamber stability with no fluctuations, Grade 4 = unstable chamber with AC collapse), the data showed that the QUATERA 700 with its advanced QUATTRO pump outperformed the two competitors for providing better anterior chamber stability. Mean chamber stability for both the soft and dense cataract subgroups, operated on with the QUATERA 700 was 1.1, indicating excellent stability with no fluctuations.
In addition, with its POD technology, the QUATERA 700 had an advantage compared to the other two systems for reducing total ultrasound time. A statistically significant difference between systems favoring the QUATERA 700 was also seen in the analysis of fluid turnover in the dense cataract subgroup (Table 2).
Our study also evaluated corneal clarity on postoperative day 1 using a scale of 0 (perfectly clear) to 4 (diffuse edema). For both the soft and dense cataract subgroups, the score was numerically better for the QUATERA 700 compared with the WHITESTAR SIGNATURE PRO and the Centurion Vision System, although the differences were not statistically significant. In addition, endothelial cell count and corneal thickness at 2 weeks after surgery was evaluated using data from 15 eyes in each of the 6 surgical subgroups. The results of those analyses also showed no statistically significant differences between phacoemulsification groups for eyes with soft or dense cataracts.


Intraoperative video from cases included in the study highlight the performance of the QUATERA 700 and differentiate it from the other units (Figure 5). The video from a case involving a patient with a grade 3 cataract shows the efficiency of removing the nuclear quadrants with the QUATERA 700 that used the highest combination of flow and vacuum rates. High vacuum enables holdability during chopping of dense cataracts, and the QUATTRO pump maintained anterior chamber stability. Viewing the video, surgeons can appreciate that there is no more than minimal anterior chamber fluctuation or movement of the iris or posterior capsule in this procedure performed with the QUATERA 700.
In contrast, evidence of surge, pupil expansion and relaxation, and chamber fluctuation with iris movement, and the development of some corneal folds were seen in videos of procedures performed with the Centurion Vision System (Figure 5). In fact, the only intraoperative complication encountered in the study involved a posterior capsule rent that occurred secondary to surge in an eye with a dense cataract operated on with the Centurion Vision System (Table 2). The eye required vitrectomy but was able to be implanted with the posterior chamber IOL in the capsular bag.
Procedures done with the WHITESTAR SIGNATURE PRO were associated with some anterior chamber fluctuation. In addition, because the WHITESTAR SIGNATURE PRO uses a lower flow rate than the QUATERA 700 (60 cc/min vs. 90 cc/min), in my experience it is less effective than the QUATERA 700 in attracting nuclear pieces to the phacoemulsification tip. As a result, the need to move the tip inside the eye to capture nuclear pieces raises concern about safety on my end.
My surgical tips for using the QUATERA 700
Considering the safety I experienced using the QUATTRO pump technology, I recommend that when experienced surgeons begin using the QUATERA 700, they can set the vacuum and aspiration flow rate to high levels. Not only do I believe that it is safe to use higher vacuum when operating with the QUATERA 700 but operating with higher vacuum makes the surgery faster and more efficient. In my hands, a high vacuum setting and aspiration rate provides great followability that allows me to keep the phacoemulsification tip in the safe zone in the center of the pupil. From my experience, enhancing safety using other machines requires using lower parameters that result in reduced efficiency. Alternatively, surgeons can choose to use a tip with an aspiration bypass system, but this equipment also compromises efficiency because it reduces holdability and followability.
I suspect, that less experienced surgeons might feel more comfortable setting vacuum to 500 mmHg when they first begin using the QUATERA 700. During their first cases performed with the QUATERA 700, my residents were setting the vacuum at 300 mmHg. Using this approach they were having to move the phacoemulsification tip out to the periphery to access nuclear fragments, which is dangerous because the anterior chamber is shallower in the periphery and the phacoemulsification tip comes closer to the posterior capsule, cornea, and iris. When my residents switched to setting the vacuum on the QUATERA 700 to 500 mmHg and followed my advice to keep the phacoemulsification tip in the center, they were more relaxed and able to enjoy themselves while performing the surgery.
Conclusion
The QUATERA 700 phacoemulsification system is built with the innovative QUATTRO pump that maintains anterior chamber stability even at higher flow and vacuum rates for enhanced safety and efficiency. It offers the new ultrasound management system POD that in my opinion further increases safety and efficiency by reducing total ultrasound usage. In addition, QUATERA 700 is part of a surgical cockpit that integrates the diagnostic and surgical equipment seamlessly and therefore enhances efficiency in my OR.






{kind=link}
{kind=link}