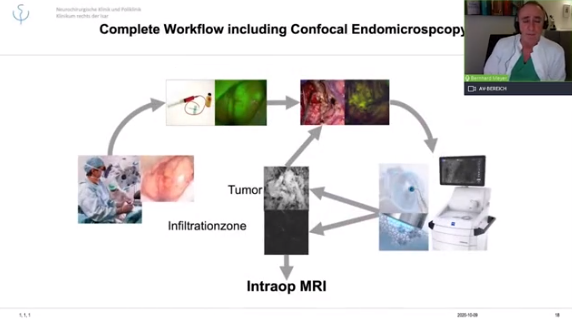
ZEISS Tumor Workflow
The ZEISS Tumor Workflow9 combines three leading technologies from ZEISS: Advanced surgical visualization, in vivo pathology, and intraoperative radiotherapy. Thereby, ZEISS supports multidisciplinary teams, including neurosurgeons, neuropathologists, and radiation oncologists, over several steps of the surgical workflow in delivering brain tumor treatment.